
Sinusitis is an inflammation of the paranasal sinuses, which may or may not be as a result of infection, from bacterial, fungal, viral, allergic or autoimmune issues. Newer classifications of sinusitis refer to it as rhinosinusitis, taking into account the thought that inflammation of the sinuses cannot occur without some inflammation of the nose as well (rhinitis).
Classification of Sinusitis
By location
There are several paired paranasal sinuses, including the frontal, ethmoid, maxillary and sphenoid sinuses. The ethmoid sinuses can also be further broken down into anterior and posterior, the division of which is defined as the basal lamella of the middle turbinate. In addition to the acuity of disease, discussed below, sinusitis can be classified by the sinus cavity which it affects:
- Maxillary sinusitis – can cause pain or pressure in the maxillary (cheek) area (e.g., toothache, headache) (J01.0/J32.0)
- Frontal sinusitis – can cause pain or pressure in the frontal sinus cavity (located behind/above eyes), headache (J01.1/J32.1)
- Ethmoid sinusitis – can cause pain or pressure pain between/behind eyes, headache (J01.2/J32.2)
- Sphenoid sinusitis – can cause pain or pressure behind the eyes, but often refers to the vertex of the head(J01.3/J32.3)
Recent theories of sinusitis indicate that it often occurs as part of a spectrum of diseases that affect the respiratory tract (i.e. – the “one airway” theory) and is often linked to asthma. All forms of sinusitis may either result in, or be a part of, a generalized inflammation of the airway so other airway symptoms such as cough may be associated with it.
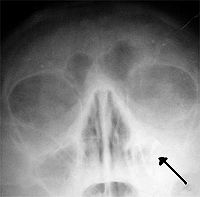
Left-sided maxillar sinusitis (Absence of the air transparency of left maxillar sinus)
By duration
Sinusitis can be acute (going on less than four weeks), subacute (4-12 weeks) or chronic (going on for 12 weeks or more).
All three types of sinusitis have similar symptoms, and are thus often difficult to distinguish.
Acute sinusitis
Acute sinusitis is usually precipitated by an earlier upper respiratory tract infection, generally of viral origin. Virally damaged surface tissues are then colonized by bacteria, most commonly Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis and Staphylococcus aureus. Other bacterial pathogens include other streptococci species, anaerobic bacteria and, less commonly, gram negative bacteria. Another possible cause of sinusitis can be dental problems that affect the maxillary sinus. Acute episodes of sinusitis can also result from fungal invasion. These infections are most often seen in patients with diabetes or other immune deficiencies (such as AIDS or transplant patients on anti-rejection medications) and can be life threatening. In type I diabetes, ketoacidosis causes sinusitis by Mucormycosis.
Chronic sinusitis
Chronic sinusitis is a complicated spectrum of diseases that share chronic inflammation of the sinuses in common. The causes are multifactorial and may include allergy, environmental factors such as dust or pollution, bacterial infection, or fungus (either allergic, infective, or reactive). Non allergic factors such as vasomotor rhinitis can also cause chronic sinus problems. Abnormally narrow sinus passages, which can impede drainage from the sinus cavities, can also be a factor.
Symptoms include: nasal congestion; facial pain; headache; fever; general malaise; thick green or yellow discharge; vertigo; blurred vision, feeling of facial ‘fullness’ or ‘tightness’ which worsens on bending over; aching teeth, and halitosis.
Very rarely, chronic sinusitis can lead to Anosmia, the inability to smell or detect odors.
In a small number of cases, chronic maxillary sinusitis can also be brought on by the spreading of bacteria from a dental infection.
Attempts have been made to provide a more consistent nomenclature 6 for subtypes of chronic sinusitis. A task force for the American Academy of Otolaryngology – Head and Neck Surgery / Foundation along with the Sinus and Allergy Health Partnership broke Chronic Sinusitis into two main divisions, Chronic Sinusitis without polyps and Chronic Sinusitis with polyps (also often referred to as Chronic Hyperplastic Sinusitis). Recent studies which have sought to further determine and characterize a common pathologic progression of disease have resulted in an expansion of proposed subtypes. Many patients have demonstrated the presence of eosinophils in the mucous lining of the nose and paranasal sinuses. As such the name Eosinophilic Mucin RhinoSinusitis (EMRS) has come into being. Cases of EMRS may be related to an allergic response, but allergy is often not documentable, resulting in further subcategorization of allergic and non-allergic EMRS.
A more recent, and still debated, development in chronic sinusitis is the role that fungus may play. Fungus can be found in the nasal cavities and sinuses of most patients with sinusitis, but can also be found in healthy people as well. It remains unclear if fungus is a definite factor in the development of chronic sinusitis and if it is, what the difference may be between those who develop the disease and those who do not.
Role of biofilms
Biofilms are complex aggregates of extracellular matrix and inter-dependent microorganisms from multiple species, many of which may be difficult or impossible to isolate using standard clinical laboratory techniques. Bacteria found in biofilms may show increased antibiotic resistance when compared to free-living bacteria of the same species. It has been hypothesized that biofilm-type infections may account for many cases of antibiotic-refractory chronic sinusitis.[1] A recent study found that biofilms were present on the mucosa of 3/4 of patients undergoing surgery for chronic sinusitis.[2]
Sinus headache vs. migraine
Headache/facial pain (characteristic of Sinusitis pain are dull, constant, aching pain over the affected frontal or sphenoid sinus area) is one of the general symptom complained during acute or chronic stages of Sinusitis (Sinusitis = tender face + coryza + post nasal drip).[3] This pain (i.e. facial pain (pressure), headache) is typically localised to the involved sinus and is worsened when the affected person bends over or when in supine position. Rarely, sphenoid or Ethmoid sinusitis causes severe frontal or retroorbital pain and advanced frontal sinusitis can present as Pott’s puffy tumour. During Acute sinusitis thick purulent nasal discharge (usually green in colour and with or without blood) and typical localised headache (toothache) are present. Whereas in Migraine (Migraine = episodic typical unilateral headache + often Vomiting + visual disturbances)[4] photo phobia, phono phobia and Triad 1. premonitory visual (scotoma or scintillations) sensory or motor symptoms, 2. unilateral throbbing headache, 3. nausea and vomiting are present.[5]
Recent studies on sinusitis and migraine
Headache is a common symptom of sinusitis and “sinus headache” rarely but can be a misdiagnosis of a migraine. Acute sinusitis can cause pressure within the sinus cavities of the head, but this typically has associated pain to palpation of the sinus area and purulent greenish discharge from the nose. The use of the term sinus headache therefore is often misleading and results in underdiagnosis of migraine. Recent studies indicate that up to 90% of “sinus headaches” are migraine[6][7] This confusion occurs in part because migraine involves activation of the trigeminal nerves which innervate both the sinus region but also the meninges which surround the brain. As a result, direct determination of the site of pain origination can be confused on a cortical level. Additionally, nasal congestion is not an uncommon result of migraine headaches, further confusing the issue. A recent study further demonstrated that most patients with “sinus headache” respond to triptan migraine medications, and state dissatisfaction with their treatment when they are treated with decongestants or antibiotics.[8] The subtlety is that while most patients with sinusitis have some sort of facial pain, pressure, or headache, not all patients who attribute the symptom of headache to their sinuses may have legitimate diseases of the sinus. Acute and chronic sinusitis can cause pressure within the sinus cavities of the head, but this is associated with pain on palpation of the sinus area.
Predisposing factors
Factors which may predispose to developing sinusitis include: allergies; structural problems such as a deviated septum or small sinus ostia; smoking; nasal polyps; carrying the cystic fibrosis gene (research is still tentative); prior bouts of sinusitis as each instance may result in increased inflammation of the nasal or sinus mucosa and potentially further narrow the openings.
Diagnosis for Sinusitis
Acute sinusitis
Usually Sinusitis is diagnosed clinically.
Clinically bacterial and Viral Acute sinusitis are difficult to distinguish however, disease duration less than 7 days is considered as a Viral whereas more than 7 days are considered as a bacterial sinusitis (usually 30% to 50% are Bacterial sinusitis).
- In suspected Acute Fungal Sinusitis – Multiple biopsy of involved area are performed to confirm etiological diagnosis.
- Nosocomial Acute sinusitis is confirmed with the help of CT scan of the sinuses.
Chronic sinusitis
In Chronic sinusitis (lasting more than 12 weeks) CT scan, tissue sample for Histology and Cultures can be used for diagnosis.
- In Chronic Bacterial sinusitis CT scan is used to define the range, extent of the disease and response of the treatment course. Tissue samples for Histology and culture is obtained to confirm a diagnosis.
- Allergic fungal sinusitis are often seen in a person with asthma and nasal polyps. Multiple Biopsy is informative to confirm the diagnosis.[5]
When imaging techniques are required for diagnosis CT scanning is the method of choice. If allergies are suspected, allergy testing may be performed.
ENT specialists utilize a procedure known as nasal endoscopy (if nasal endoscopy is indicated) to diagnose sinus infection. This involves inserting a flexible fiber-optic tube with a light and camera at its tip into the nose to examine the nasal passages and sinuses. This is generally a completely painless procedure which takes between 5 to 10 minutes to complete.
Treatment of Sinusitis
Acute sinusitis
There are over the counter medicines that can relieve some of the symptoms associated with sinusitis, such as headaches, pressure, fatigue and pain. Usually these are a combination of some kind of antihistamine along with decongestant or pain reliever. Seeing a doctor will usually result in a prescription for antibiotics and a recommendation for rest.
Therapeutic measures range from the medicinal to the traditional and may include nasal irrigation or jala neti using a warm saline solution, hot drinks including tea and chicken soup, over-the-counter decongestants and nasal sprays, and getting plenty of rest. Analgesics (such as aspirin, paracetamol (acetaminophen) or ibuprofen) can be used, but caution must be employed to make sure the patient does not suffer from aspirin-exacerbated respiratory disease (AERD) as this could lead to anaphylaxis.
If sinusitis doesn’t improve within 48 hours, or is causing significant pain, a doctor may prescribe antibiotics (Amoxicillin usually being the most common) with amoxicillin/clavulanate (Augmentin/Co-Amoxiclav) being indicated for patients who fail amoxicillin alone. Fluoroquinolones, and less frequently Doxycycline are used in patients who are allergic to penicillins.
A recent British study has found that for most cases of acute sinusitis, antibiotics and nasal corticosteroids work no better than a placebo.[9]
Chronic sinusitis
Simple measures
Nasal irrigation and flush promotes sinus cavity health, and patients with chronic sinusitis including symptoms of facial pain, headache, halitosis, cough, anterior rhinorrhea (watery discharge) and nasal congestion found nasal irrigation to be “just as effective at treating these symptoms as the drug therapies.” In other studies, “daily hypertonic saline nasal irrigation improves sinus-related quality of life, decreases symptoms, and decreases medication use in patients with frequent sinusitis,” and is “recommended as an effective adjunctive treatment of chronic sinonasal symptoms.”[10][11][12]
Some people use bulb syringes, squirt bottles, and neti pots. Others use pulsating irrigation devices that deliver an intermittent pulsing saline rinse to remove bacteria, purulent material, and help restore ciliary function.
Some published medical reports indicate pulsatile lavage is more effective at cleansing and removing bacteria than non-pulsating nasal wash products like bulb syringes, neti pots and squeeze bottles, which rely simply on gravity and conventional flow.[13][14][15]
A pulsating nasal irrigation device delivers a controlled flow with pressure control that may be adjusted for individual comfort. Medical reports support that positive pressure irrigation retains a larger volume of solution and irrigates the sinuses more consistently than other methods.[16]
Medical approaches
For chronic or recurring sinusitis, referral to an otolaryngologist (also called an “ear-nose-and-throat” doctor or ENT) may be indicated for more specialist assessment and treatment, which may include nasal surgery. However, for most patients the surgical approach is not superior to appropriate medical treatment. Surgery should only be considered for those patients who do not experience sufficient relief from optimal medication.[17][18]
A relatively recent advance in the treatment of sinusitis is a type of surgery called functional endoscopic sinus surgery (FESS), whereby normal clearance from the sinuses is restored by removing the anatomical and pathological obstructive variations that predispose to sinusitis. This replaces prior open techniques requiring facial or oral incisions and refocuses the technique to the natural openings of the sinuses instead of promoting drainage by gravity, the idea upon which the Caldwell-Luc surgery was based.[1]
Another recently developed treatment is balloon sinuplasty. This method, similar to balloon angioplasty used to “unclog” arteries of the heart, utilizes balloons in an attempt to expand the openings of the sinuses in a less invasive manner. Its final role in the treatment of sinus disease is still under debate but appears promising.
Based on the recent theories on the role that fungus may play in the development of chronic sinusitis, newer medical therapies include topical nasal applications of antifungal agents. Much of the original research indicating fungus took place at the Mayo Clinic and they have since patented this treatment option.[19] Although there are some licensing battles taking place over these drugs as a result of the patent, they are currently available for other uses and therefore can be compounded by pharmacies or even by the patient.
Surgical approach and treatment
A number of surgical approaches can be used, either by endoscopy or conventional incision generally through nose or mouth.
- Endoscopic nasal Surgery allows more functional approach than by radical antrostomy.
- Intranasal endoscopic operations permits minimal trauma to adjacent tissues and precise removal of the diseased mucosa.
If fibrosis of the antrum is present (natural ostium can be completely obstructed) by infection and inflammation; intranasal inferior meatal antrostomy can be used to ease drainage from the antrum. Or, intranasal indoscopic techniques can be used to create a middle meatal antrostomy (e.g. middle turbinate is lifted and infundibulum is localised and enlarged anteriorly, generally excision of anterior end of the unicate process is not required, antrum can be inspected through antrostomy by the use of 30 and 70 degree rigid endoscopy.)
For persisting Sinusitis Caldwell-Luc radical antrostomy can be used (e.g. incision in the upper gum, opening in the anterior wall of the antrum, removal of the entire diseased maxillary sinus mucosa and drainage is allowed into inferior meatus by creating a large window in the lateral nasal wall.)[20]
Once incissional entry is gained into the paranasal sinus, surgery can be extended to another sinus or other adjacent anatomical structures. e.g. internal maxillary artery, pterygopalatine fossa and sphenopalatine ganglion.
Other approaches
Phage therapy: Since the discovery of spontaneous bacterial lysis (from bacteriophages) by Frederick Twort and by Felix d’Herelle, phage therapy (treatment with bacterial viruses) has been used extensively with miscellaneous bacterial infections in the areas of otolaryngology, stomatology, ophthalmology, dermatology, pediatrics, gynecology, surgery (especially against wound infections), urology, and pulmonology.[21][22][23] Treatment with phages was developed in the Soviet Union in parallel to the western development of antibiotics. Currently phage therapy for chronic Sinusitis is available at the Phage Therapy Center, Tbilisi, Republic of Georgia,[24] or in Poland.[25]
Homeopathy Treatment for Sinusitis
Keywords: homeopathy, homeopathic, treatment, cure, remedy, remedies, medicine
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines are selected after a full individualizing examination and case-analysis, which includes the medical history of the patient, physical and mental constitution, family history, presenting symptoms, underlying pathology, possible causative factors etc. A miasmatic tendency (predisposition/susceptibility) is also often taken into account for the treatment of chronic conditions. A homeopathy doctor tries to treat more than just the presenting symptoms. The focus is usually on what caused the disease condition? Why ‘this patient’ is sick ‘this way’. The disease diagnosis is important but in homeopathy, the cause of disease is not just probed to the level of bacteria and viruses. Other factors like mental, emotional and physical stress that could predispose a person to illness are also looked for. No a days, even modern medicine also considers a large number of diseases as psychosomatic. The correct homeopathy remedy tries to correct this disease predisposition. The focus is not on curing the disease but to cure the person who is sick, to restore the health. If a disease pathology is not very advanced, homeopathy remedies do give a hope for cure but even in incurable cases, the quality of life can be greatly improved with homeopathic medicines.
The homeopathic remedies (medicines) given below indicate the therapeutic affinity but this is not a complete and definite guide to the homeopathy treatment of this condition. The symptoms listed against each homeopathic remedy may not be directly related to this disease because in homeopathy general symptoms and constitutional indications are also taken into account for selecting a remedy. To study any of the following remedies in more detail, please visit the Materia Medica section at Hpathy.
None of these medicines should be taken without professional advice and guidance.
Homeopathy Remedies for Sinusitis :
Ars., berb., bry., calc., cinnb., cupr., ferr., hydr., kali-bi., kali-chl., kali-i., kali-s., lach., lyc., med., merc., merc-i-f., nat-s., nux-v., ph-ac., phos., puls., pyrog., sang., sil., spig., stict., teucr., thuj., verb.
References
- Ramadan H, Sanclement J, Thomas J (2005). “Chronic rhinosinusitis and biofilms.”. Otolaryngol Head Neck Surg 132 (3): 414–7. doi:. PMID 15746854.
- Bendouah Z, Barbeau J, Hamad W, Desrosiers M (2006). “Biofilm formation by Staphylococcus aureus and Pseudomonas aeruginosa is associated with an unfavorable evolution after surgery for chronic sinusitis and nasal polyposis.”. Otolaryngol Head Neck Surg 134 (6): 991–6. doi:. PMID 16730544.
