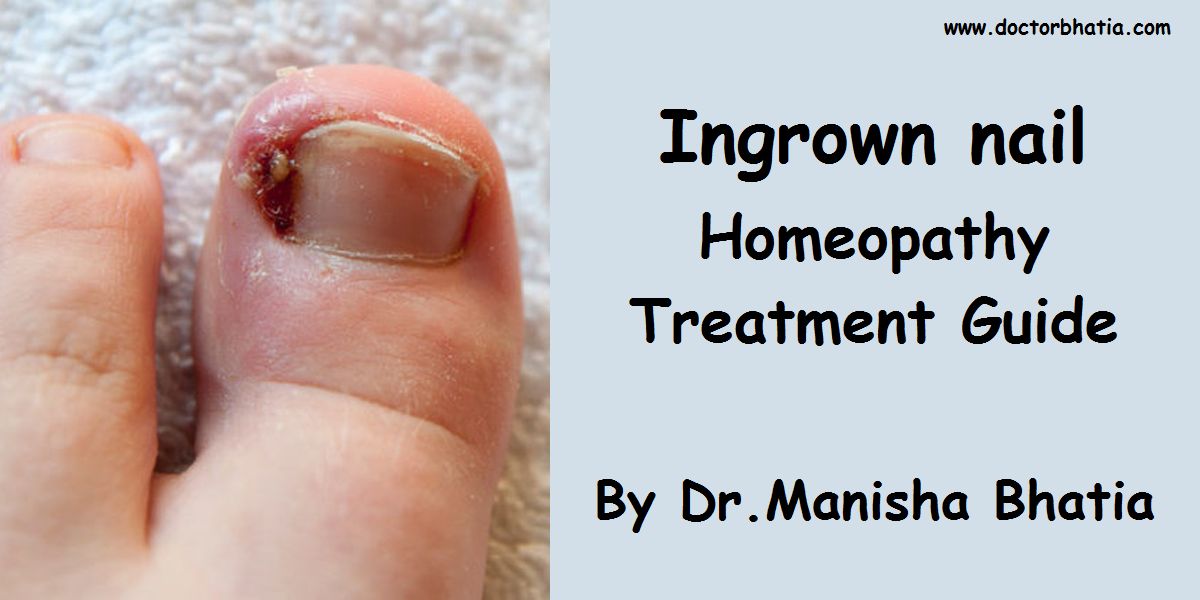
Onychocryptosis, commonly known as ingrown nails (unguis incarnatus) or ingrowing nails, is a common form of nail disease. It is an often painful condition in which the nail grows or cuts into one or both sides of the nail bed. While ingrown nails can occur in both the nails of the hand and feet, they occur most commonly with toenails.
Causes of Ingrown nail
Causes include:
- bad maintenance [like cutting the nail too short, rounded off at the tip or peeled off at the edges (versus being cut straight across)];[1]
- ill-fitting shoes [those that are too narrow or too short can cause bunching of the toes in the developmental stages of the foot (frequently in those under 21), causing the nail to curl and dig into the skin];
- trauma to the nail plate or toe [which can occur by stubbing the toenail, dropping things on the toe and ‘going through the end of your shoes’ during sports, can cause the flesh to become injured and the nail to grow irregularly and press into the flesh]; and
- predisposition [abnormally shaped nail beds, nail deformities caused by diseases, and a genetic susceptibility to nail problems can mean a tendency to ingrowth].
Symptoms of Ingrown nail
Chronically ingrown toenail (that twice had failed wedge resections on both sides)
Symptoms of an ingrown nail include pain along the margins of the nail (caused by hypergranulation that occurs around the aforementioned region), worsening of pain when wearing shoes or other tight articles, and sensitivity to pressure of any kind, even the weight of bed sheets or a duvet. Bumping of an affected toe with objects can produce sharp, even excruciating, pain as the tissue is punctured further by the ingrown nail. By the very nature of the condition, ingrown nails become easily infected unless special care is taken to treat the condition early on and keep the area as clean as possible. Signs of infection include redness and swelling of the area around the nail, drainage of pus and watery discharge tinged with blood. The main symptom is swelling at the base of the nail on whichever side (if not both sides) the ingrowing nail is forming.
If left untreated
If an ingrown nail is left untreated, there exists a high risk of dangerous infection. When the skin around the nail gets infected, it begins to swell up and put even more pressure against the nail. Ingrown nails can produce a spear shaped wedge of nail on the lateral side of the toe which will progressively become more embedded into the toe tissue as the nail grows forward. In the worst case, the swelling will begin putting sideways pressure on the nail, causing it to grow at a slant. This will cause both sides of the nail to eventually become ingrown and swollen. Eventually the swollen parts of the skin will begin to harden and fold over the nail. An untreated ingrown toenail will cause a person to walk with a limp, which over a long period of time may cause further pain and injury to the foot, leg and back owing to improper distribution of weight. Other non-direct effects of seriously ingrown nails include lack of exercise, constant and unrelenting pain and pressure which is often extreme and debilitating when weight has been on the foot for an extended period of time, the spread of infection, loss of appetite, inability to move around, and psychological effects (like anxiety, stress and feelings of despair). Amputation of the toe, foot or leg may be the final outcome if the infection is left untreated long enough for gangrene to set in as a result of a foot ulcer, most common on people with diabetes. An untreated infection may also lead to a condition known as osteomyelitis, where the infection spreads to the bone of the infected digit. Once in the bone, the infection is more difficult to remove and may require the intravenous treatment of antibiotics. One should always consult a doctor when infection is present.
The scenarios described above are “worst case”. Many ingrown toenails do not progress to an infection, and sometimes they heal themselves without intervention. However, a visit to a podiatrist is recommended if swelling is severe, if there is pus, or if the toenail remains ingrown for more than a few months.
Prevention for Ingrown nail
The most common place for ingrown nails is in the big toe, but ingrowth can occur on any nail. Ingrown nails can be avoided by cutting nails straight across; nails should not be cut along a curve, nor should they be cut too short. In both cases, the important thing to avoid is cutting the nail shorter than the flesh around it. Footwear which is too small, either in size or width, or those with too shallow a ‘toe box’ will exacerbate any underlying problem with a toenail.
Ingrown toe nails can be caused by injury, commonly concussion where the flesh is pressed against the nail causing a small cut that swells. Also, injury to the nail can cause it to grow abnormally, making it thicker or wider than normal or even bulged or crooked. Stubbing the toenail, dropping things on the toe and ‘going through the end of your shoes’ in sports are common injuries to the digits. Injuries to the toes can be prevented by wearing shoes most of the time, especially when working or playing.
One myth is that a V should be cut in the end of the ingrown nail; this myth is untrue. The reasoning of the myth is that if one cuts a V in the nail, the edge of the nail will grow together as the nail grows out. This does not happen – the shape of the nail is determined by the growing area at the base of the toe and not by the end of the nail. A notch does no good, and may do harm if it is cut too deeply.[1]
Treatment of Ingrown nail
Treatment of ingrown nails ranges from soaking the afflicted area to surgery. The appropriate method is dictated by the severity of the condition. In nearly all cases, drainage of blood or watery discharge should mean a trip to the doctor, usually a podiatrist, a specialist trained explicitly to treat these conditions. Most practitioners agree that trying to outwait the condition is nearly always fruitless, as well as agonizing.
Home care
In mild cases (not including the severe cases as in the photos above), doctors recommend daily soaking of the afflicted digit in a mixture of warm water and Epsom salts and applying an over-the-counter antiseptic. This might allow the nail to grow out so it may be trimmed properly and the flesh to heal. Note that infection may be somewhat difficult to prevent in cleaning and treating ingrown nails owing to the warm, dark, and damp environment in shoes. Peroxide is immediately effective to help clean minor infections but iodine is more effective in the long term as it continues to prevent bacterial growth even after it is dry. [N.B.: Iodine should not be used on deep wounds. In such cases a physician or podiatrist should be consulted.] Also, bandages can help keep out bacteria. [N.B. One should never apply any of the new types of spray-on bandages to ingrown nails that show any discharge – preventing drainage will likely cause intense swelling and pain. Removal of spray-on bandages can be achieved with common rubbing alcohol.]
Some doctors in the very early stages of an ingrown toenail will apply silver nitrate to prevent further growth.
It is also advisable to walk around barefoot so that air has a chance to circulate. Infections often become more painful when they are not exposed to air because bacteria grows more quickly in warmer conditions e.g. when the foot is impacted tightly in a shoe.
These home remedies are, in serious cases, ineffective: when the flesh is far too swollen and infected these procedures will not work. Thus, these more severe cases, such as when the area around the nail becomes infected or the nail will not grow back properly, must be treated by a professional and the patient should avoid repeated attempts at this type of ‘bathroom surgery.’

Toothpick segment as home remedy to prevent ingrowing.
Phenolisation
Following injection of a local anaesthetic at the basis of the toenail and perhaps application of a tourniquet, the surgeon will remove (ablate) the edge of the nail growing into the flesh and destroy the matrix area with phenol to permanently and selectively ablate the matrix that is manufacturing the ingrown portion of the nail (i.e., the nail margin). This is known as a partial matrixectomy, phenolisation, phenol avulsion or partial nail avulsion with matrix phenolisation. Also, any infection is surgically drained. After this procedure, other suggestions on aftercare will be made, such as salt water bathing of the digit in question. The point of the procedure is that the nail does not grow back where the matrix has been cauterized and so the chances of further ingrowth are very low. The nail is slightly (usually one millimeter or so) narrower than prior to the procedure and is barely noticeable one year later. The surgery is advantageous because it can be performed in the doctor’s office under local anesthesia with minimal pain following the intervention. Also, there is no visible scar on the surgery site and a nominal chance of recurrence.
Wedge Resection
Partial removal of the nail or an offending piece of nail. More complex than a complete nail avulsion (removal).
Here, the digit is first injected with a common local anesthetic. When the area is numb, the physician will perform an onychotomy in which the nail along the edge that is growing into the skin is cut away (ablated) and the offending piece of nail is pulled out. Any infection is surgically drained. This process is referred to as a “wedge resection” or simple surgical ablation and is non-permanent (i.e., the nail will re-grow from the matrix). The entire procedure may be performed in a physician’s office and takes approximately thirty to forty-five minutes depending on the extent of the problem. The patient is allowed to go home immediately and the recovery time is anywhere from a few days to a week barring any complications such as infection. As a followup, a physician may prescribe an oral or topical antibiotic or a special soak to be used for approximately a week after the surgery.

A resected wedge from the left side of the left big toe, shown to scale.
It should be noted that some physicians will not perform a complete nail avulsion (removal) under any but the most extreme circumstances. In most cases, these physicians will remove both sides of a toenail (even if one side is not currently ingrown) and coat the nail matrix on both of those sides with a chemical or acid (usually phenol) to prevent re-growth. This leaves the majority of the nail intact, but ensures that the problem of ingrowth will not re-occur.
Disadvantages: If the nail matrix is not coated with the applicable chemical or acid (phenol) and is allowed to re-grow, this method is prone to failure. Also, the underlying condition can still become symptomatic as the nail grows out over the course of up to a year: the nail matrix might be manufacturing a nail that is simply too curved, thick, wide or otherwise irregular to allow for normal growth. Furthermore, the flesh can be injured very easily by concussion, tight socks, quick twisting motions while walking or just the fact the nail is growing wrongly (likely too wide). This hypersensitivity to continued injury can mean chronic ingrowth; the solution is nearly always edge avulsion by the highly successful phenolisation.

Post-surgery toe with removed nail shard
Recurrence: If the nail becomes ingrown again after a wedge resection more invasive surgery is required. This can often include the destruction of the nail bed. This surgery takes longer than the minor wedge resection. During it the toe will be torniqued and incisions will be made from the front of the toe to around 1cm behind the rear of the visible part of the nail. These incisions are quite deep and will require stitching and will also scar. The nail will then be cut out, much like a wedge resection and the nail bed broken to prevent regrowth. The nail will be significantly narrower after this surgery and may appear visibly deformed but will not become ingrown again. Note: if undertaking this surgery it is advisable to leave at least 4 days before walking any further than very short distances as even with painkillers this can be exceedingly painful. It is also important if you are required by your employer to stand for extended periods of time that they be made aware you may be unable to work for 1-2 weeks (at most) depending on your speed of recovery.
CO2 Laser surgery
Following injection of a local anaesthetic at the basis of the toe and perhaps application of a small tourniquet, the surgeon will remove (ablate) the edge of the nail growing into the flesh and cauterize the matrix area by laser photocoagulation. This too is known as a partial matrixectomy or partial nail avulsion. Here too, the point of the procedure is that the nail does NOT grow back where the matrix has been cauterized and so the chances of further ingrowth is very low. The nail is slightly (usually one millimeter or so) narrower than prior to the procedure. Disadvantages: sutures are usually necessary, post-operative pain due to the wound and scar.
Nail Avulsion
Nail avulsion (or removal) of whole nail does not always prevent recurrences. In case of recurrence in spite of complete removal, and if the patient never feels any pain before inflammation occurs, the condition is more likely to be onychia which is often confused for an ingrown or ingrowing nail (onychocryptosis).
Complete removal of whole nail is a simple procedure. Here, anaesthetic is injected, the nail is removed quickly and painlessly and the patient can leave immediately. The entire procedure can be performed in around 10 minutes and is much less complex than a “wedge resection” as above. Note that the nail will grow back. However, in most cases it will cause further problems as it can become ingrown very easily as the nail grows outward. It can become easily injured by concussion and in some cases grows back too thick, too wide or deformed. This procedure can thus result in chronic ingrown nails and is therefore considered a generally unsuccessful solution, especially considering the pain involved.
Accordingly, in some cases as determined by a doctor, the nail matrix is coated with a chemical (usually phenol) so none of the nail will ever grow back. This is known as a permanent or full nail avulsion, or full matrixectomy, phenolisation, or full phenol avulsion. As can be seen in the images below, the nail-less toe looks much like a normal toe and fake nails or nail varnish can still be applied to the area.

Homeopathy Treatment for Ingrown nail
Keywords: homeopathy, homeopathic, treatment, cure, remedy, remedies, medicine
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines are selected after a full individualizing examination and case-analysis, which includes the medical history of the patient, physical and mental constitution, family history, presenting symptoms, underlying pathology, possible causative factors etc. A miasmatic tendency (predisposition/susceptibility) is also often taken into account for the treatment of chronic conditions. A homeopathy doctor tries to treat more than just the presenting symptoms. The focus is usually on what caused the disease condition? Why ‘this patient’ is sick ‘this way’. The disease diagnosis is important but in homeopathy, the cause of disease is not just probed to the level of bacteria and viruses. Other factors like mental, emotional and physical stress that could predispose a person to illness are also looked for. No a days, even modern medicine also considers a large number of diseases as psychosomatic. The correct homeopathy remedy tries to correct this disease predisposition. The focus is not on curing the disease but to cure the person who is sick, to restore the health. If a disease pathology is not very advanced, homeopathy remedies do give a hope for cure but even in incurable cases, the quality of life can be greatly improved with homeopathic medicines.
The homeopathic remedies (medicines) given below indicate the therapeutic affinity but this is not a complete and definite guide to the homeopathy treatment of this condition. The symptoms listed against each homeopathic remedy may not be directly related to this disease because in homeopathy general symptoms and constitutional indications are also taken into account for selecting a remedy. To study any of the following remedies in more detail, please visit the Materia Medica section at Hpathy.
None of these medicines should be taken without professional advice and guidance.
Homeopathy Remedies for Ingrown nail :
Alum., caust., colch., graph., kali-c., kali-khl., mag-aust., nat-m., nit-ac., ph-ac., plb., sil., sulph., teucr., thuj., tub.
Footnotes
- ^ “Ingrown Toenail“. Retrieved on 2008-03-19.
References
- Aksakal, A. B., E. Ozsoy, et al (2003). “Silicone gel sheeting for the management and prevention of onychocryptosis.” Dermatol Surg 29(3): 261-4.
- Boll OF. Surgical correction of ingrowing toenails. J Natl Assoc Chiroprod. 1945; 35:8-9.
- Kominsky, S. J. and M. D. Daniels (2000). “A modified approach to the phenol and alcohol chemical partial matrixectomy.” J Am Podiatr Med Assoc 90(4): 208-10.
- Rounding C, Bloomfield S. Surgical treatment for ingrowing toenails (Cohrane Review). In: The Cochrane Library, Issue 4, 2004. Chichester, UK: John Wiley & Sons, Ltd.
- Boberg JS & al. Scientific analysis of phenol nail surgery. J Am Podiatr Med Assoc 2002;92(10):575-9
