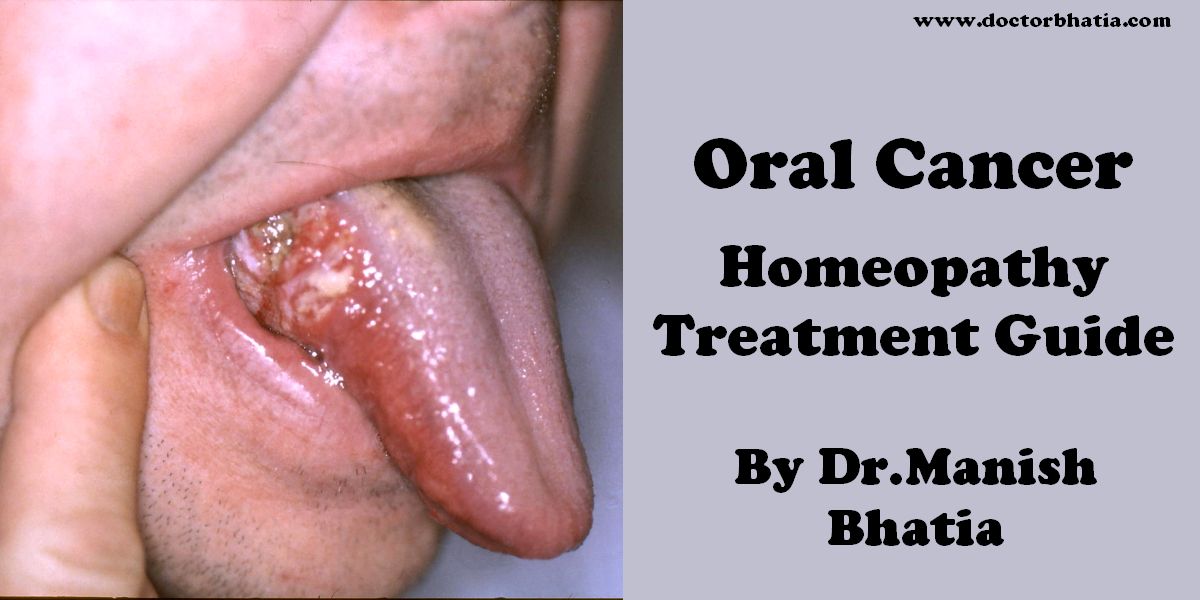
Oral cancer is any cancerous tissue growth located in the mouth. It may arise as a primary lesion originating in any of the oral tissues, by metastasis from a distant site of origin, or by extension from a neighboring anatomic structure, such as the nasal cavity or the maxillary sinus. Oral cancers may originate in any of the tissues of the mouth, and may be of varied histologic types: teratoma, adenocarcinoma derived from a major or minor salivary gland, lymphoma from tonsillar or other lymphoid tissue, or melanoma from the pigment producing cells of the oral mucosa. Far and away the most common oral cancer is squamous cell carcinoma, originating in the tissues that line the mouth and lips. Oral or mouth cancer most commonly involves the tissue of the lips or the tongue. It may also occur on the floor of the mouth, cheek lining, gingiva (gums), or palate (roof of the mouth). Most oral cancers look very similar under the microscope and are called squamous cell carcinoma. These are malignant and tend to spread rapidly.
Known risk factors
In 2008, in the US alone, about 34,000 individuals will be diagnosed with oral cancer. 66% of the time these will be found as late stage three and four disease. Low public awareness of the disease is a significant factor, but these cancers could be found at early highly survivable stages through a simple, painless, 5 minute examination by a trained medical or dental professional.
All cancers are diseases of the DNA in the cancer cells. Oncogenes are activated as a result of mutation of the DNA. The exact cause is often unknown. Risk factors that predispose a person to oral cancer have been identified in epidemiological studies.
Smoking and other tobacco use are associated with about 75 percent of oral cancer cases, caused by irritation of the mucous membranes of the mouth from smoke and heat of cigarettes, cigars, and pipes. Tobacco contains over 19 known carcinogens, and the combustion of it, and by products from this process, is the primary mode of involvement. Use of chewing tobacco or snuff causes irritation from direct contact with the mucous membranes.
In many Asian cultures chewing betel, paan and Areca is known to be a strong risk factor for developing oral cancer. In India where such practices are common, oral cancer represents up to 40% of all cancers, compared to just 4% in the UK.
Alcohol use is another high-risk activity associated with oral cancer. There is known to be a strong synergistic effect on oral cancer risk when a person is both a heavy smoker and drinker. Their risk is greatly increased compared to a heavy smoker, or a heavy drinker alone.
Some oral cancers begin as leukoplakia a white patch (lesion), red patches, (erythroplakia) or non healing sores that have existed for more than 14 days. In the US oral cancer accounts for about 8 percent of all malignant growths. Men are affected twice as often as women, particularly men older than 40/60. In Indian subcontinent Oral Submucous Fibrosis is very common.This condition is characterized by limited opening of mouth and burning sensation on eating of spicy food. This is a progressive lesion in which the opening of the mouth becomes progressively limited, and later on even normal eating becomes difficult. It occurs almost exclusively in India and Indian communities living abroad.
Human Papilloma Virus, (HPV) particularly versions 16 and 18 (there are over 100 varieties) is a known risk factor and independent causative factor for oral cancer. (Gilsion et.al.Johns Hopkins) A fast growing segment of those diagnosed does not present with the historic stereotypical demographics. Historically that has been people over 50, blacks over whites 2 to 1, males over females 3 to 1, and 75% of the time people who have used tobacco products or are heavy users of alcohol. This new and rapidly growing sub population between 20 and 50 years old is predominantly non smoking, white, and females slightly outnumber males. Recent research from Johns Hopkins indicates that HPV is the primary risk factor in this new population of oral cancer victims. HPV16/18 is the same virus responsible for the vast majority of all cervical cancers and is the most common sexually transmitted infection in the US. Oral cancer in this group tends to favor the tonsil and tonsillar pillars, base of the tongue, and the oropharnyx. Recent data suggest that individuals that come to the disease from this particular etiology have some slight survival advantage.
Symptoms of Oral cancer
Skin lesion, lump, or ulcer:
- On the tongue, lip, or other mouth area
- Usually small
- Most often pale colored, may be dark or discolored
- Early sign may be a white patch (leukoplakia) or a red patch (erythroplakia) on the soft tissues of the mouth
- Usually painless initially
- May develop a burning sensation or pain when the tumor is advanced
Additional symptoms that may be associated with this disease:
- Tongue problems
- Swallowing difficulty
- Mouth sores that do not resolve in 14 days
- Pain and paraesthesia are late symptoms.
Signs and tests for Oral cancer
An examination of the mouth by the health care provider or dentist shows a visible and/or palpable (can be felt) lesion of the lip, tongue, or other mouth area. As the tumor enlarges, it may become an ulcer and bleed. Speech/talking difficulties, chewing problems, or swallowing difficulties may develop, particularly if the cancer is on the tongue.
While a dentist, physician or other medical professional may suspect a particular lesion is malignant, the only definitive method for determining this is through biopsy and microscopic evaluation of the cells in the removed sample. A tissue biopsy, whether of the tongue or other oral tissues, and microscopic examination of the lesion confirm the diagnosis of oral cancer.
Treatment of Oral cancer
Surgical excision (removal) of the tumor is usually recommended if the tumor is small enough, and if surgery is likely to result in a functionally satisfactory result. Radiation therapy is often used in conjunction with surgery, or as the definitive radical treatment, especially if the tumour is inoperable.
Owing to the vital nature of the structures in the head and neck area, surgery for larger cancers is technically demanding. Reconstructive surgery may be required to give an acceptable cosmetic and functional result. Bone grafts and surgical flaps such as the radial forearm flap are used to help rebuild the structures removed during excision of the cancer.
Survival rates for oral cancer depend on the precise site, and the stage of the cancer at diagnosis. Overall, survival is around 50% at five years when all stages of initial diagnosis are considered. Survival rates for stage 1 cancers are 90%, hence the emphasis on early detection to increase survival outcome for patients.
Following treatment, rehabilitation may be necessary to improve movement, chewing, swallowing, and speech. Speech therapists may be involved at this stage.
Chemotherapy is useful in oral cancers when used in combination with other treatment modalities such as radiation therapy. It is seldom used alone as a monotherapy. When cure is unlikely it can also be used to extend life and can be considered palliative but not curative care. Biological agents, such as Cetuximab have recently been shown to be effective in the treatment of squamous cell head and neck cancers, and are likely to have an increasing role in the future management of this condition when used in conjunction with other treatments.
Treatment of oral cancer will usually be by a multidisciplinary team, with treatment professionals from the realms of radiation, surgery, chemotherapy, nutrition, dental professionals, and even psychology all possibly involved with diagnosis, treatment, rehabilitation, and patient care.
Homeopathy Treatment for Oral cancer
Keywords: homeopathy, homeopathic, treatment, cure, remedy, remedies, medicine
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines are selected after a full individualizing examination and case-analysis, which includes the medical history of the patient, physical and mental constitution, family history, presenting symptoms, underlying pathology, possible causative factors etc. A miasmatic tendency (predisposition/susceptibility) is also often taken into account for the treatment of chronic conditions. A homeopathy doctor tries to treat more than just the presenting symptoms. The focus is usually on what caused the disease condition? Why ‘this patient’ is sick ‘this way’. The disease diagnosis is important but in homeopathy, the cause of disease is not just probed to the level of bacteria and viruses. Other factors like mental, emotional and physical stress that could predispose a person to illness are also looked for. No a days, even modern medicine also considers a large number of diseases as psychosomatic. The correct homeopathy remedy tries to correct this disease predisposition. The focus is not on curing the disease but to cure the person who is sick, to restore the health. If a disease pathology is not very advanced, homeopathy remedies do give a hope for cure but even in incurable cases, the quality of life can be greatly improved with homeopathic medicines.
The homeopathic remedies (medicines) given below indicate the therapeutic affinity but this is not a complete and definite guide to the homeopathy treatment of this condition. The symptoms listed against each homeopathic remedy may not be directly related to this disease because in homeopathy general symptoms and constitutional indications are also taken into account for selecting a remedy. To study any of the following remedies in more detail, please visit the Materia Medica section at Hpathy.
None of these medicines should be taken without professional advice and guidance.
Homeopathy Remedies for Oral cancer :
Aur., hydr.
Complications for Oral cancer
- Postoperative disfigurement of the face, head and neck
- Complications of radiation therapy, including dry mouth and difficulty swallowing
- Other metastasis (spread) of the cancer
